


Mirza Hammad ul-Haq1Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â BDS
Sarwat Memon2Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â BDS, FCPS
Durreshahwar Agha3Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â BDS
OBJECTIVE:
The aim of this study was to compare three methods of gonial angle determination on a cephalogram with the method used to find gonial angle in an orthopantomogram, amongst three vertical groups (i.e; hyperdivergent, normodivergent and hypodivergent).
Methodology: A total of 178 panoramic and cephalometric radiographs of patients ranging from age 12-39 were used in this study. Gonial angle was constructed by three methods defined by Tweed’s, Steiner’s and Down’s on the cephalogram and was then compared to the method of gonial angle determination on an OPG. Repeated measure ANOVA with Bonferroni correction was used for comparison.
Results: The mean – difference between the values of different methods of finding Gonial Angle on cephalogram and orthopantomogram of was found to be statistically significant (i.e; P = <0.05) after Bonferroni correction amongst three vertical groups
CONCLUSION: The value of gonial angle determination on an Orthopantomogram was found to be different when compared with the three methods (Tweed’s, Steiner’s and down’s) of gonial angle determination on lateral cephalogram.
KEY WORDS: Gonial Angle, Lateral Cephalogram, Orthopantomogram, Vertical facial group.
HOW TO CITE: Ul Haq MH, Memon S, Agha D. Comparison between three methods of gonial angle formation on lateral cephalogram and orthopantomogram. J Pak Dent Assoc 2018;27(2):57-61.
DOI: https://doi.org/10.25301/JPDA.272.57
Received: 03 January 2018, Accepted: 31 January 2018
INTRODUCTION
rthodontic diagnosis is set of complex clinical expertise that requires radical data collection through diagnostics aids such as observational efficacy, clinical examinations and evaluation of records; that may not be restricted to clinical images, preliminary cast and radiographs.1,2,3 Since the emergence of cephalometric radiology in orthodontics in 1934, it has been a mainstay of comprehensive orthodontic diagnosis and also have proved worthy in determining the treatment objectives of the patients.1,3 Analysis of a cephalogram is carried upon its tracing which deduce the information on the radiograph to an attainable level.1Anatomic and derived landmarks are designated on these tracings that allows the use of a cephalogram for quantitative and qualitative analysis.3 Gonion is one of the derived landmark that is formed by bisecting the angle formed by lines tangent to the posterior border of the ramus and inferior border of the mandible or mandibular plane.4 The gonial angle also referred as the mandibular angle is the angle formed by these two above mentioned tangents.5There is a little disagreement between orthodontic analysts on the determination of mandibular plane. Depending on these differences, three of the most commonly constructed mandibular planes are:
- Down’s: line connecting Gonion(GO) and Menton(Mn)6 . Steiner’s: line connecting Gonion(GO) and Gnathion(Gn)7
- Tweed’s: tangent to the lower border of the mandible3
Because of these differences, derivation of gonial angle also differs depending upon the relative mandibular plane used.3
Gonial angle shows a great amount of individual variation based on age and type of malocclusion. It also has a key role in forensic sciences, as it can be used to asses age in extreme situations (i.e; mass destruction, murderous mutilation, missing individuals, etc.).8,9 Gonial angle has a key role during cephalometric analysis as it gives a valuable guideline to predict growth pattern and rotation of the mandible. In hyperdivergent or high angle cases the gonial angle tends to be increased (i.e; obtuse), which is depicted by downward and backward rotation of the mandible. On the contrary values of gonial angle in hypodivergent or low angle individuals tend to be decreased (i.e; acute), depicted by upward and forward rotation of the mandible.3,10,11
Hence, information provided by gonial angle is important in determining treatment objectives in orthodontic and surgical cases.3 Therefore, accurate determination of gonial angle is essential during assessment of an orthodontic case. Larheim TA, et. al (1986), found that gonial angle determination on a lateral cephalogram is unpredictable due to superimposition of images of bilateral structures. This is because a cephalogram is a 2-D illustration of a 3-D structure (i.e; skull). Conversely, gonial angle determination on a panoramic radiograph is near to that measured on dried human mandibles.12 Another advantage of an orthopantomogram is that it portrays and allows to analyze both, right and left gonial angles.3,13 According to Mattila et. al (1977), determination of gonial angle from an orthopantomogram was as accurate as from a lateral cephalogram.14
This study was conducted to find the agreement between three methods of gonial angle determination on a cephalogram and average of gonial angle on an orthopantomogram, amongst three vertical groups. (i.e; hyperdivergent, normodivergent and hypodivergent).
METHODOLOGY
A total of 178 patients seeking treatment in the Department of Orthodontics in Ziauddin College of Dentistry were included in this cross-sectional study which was conducted from March to October 2017. There were 54 males and 124 females with ages ranging from 12 to 39 years. Orthopantomograms and lateral cephalograms obtained for orthodontic purposes were used for this study. They were further divided into three groups according to their vertical skeletal pattern, depending upon the angle formed by mandibular plane (Go – Me) to the Sella- Nasion plane (SN) on lateral cephalogram: i.e; Hypodivergent <= 30o, Normodivergent > 30o – < 38o, Hyperdivergent >= 38o. Patients with a previous history of surgeries, trauma or syndromes affecting the jaws were excluded from this study. WHO sample size estimation calculator was used to calculate the sample size using means and standard deviations from a pilot study done by the principal examiner on a sample of 45 subjects (15 in each vertical group i.e. hyperdivergent, normodivergent and hypodivergent). A sample size of 178 gave the power of > 80%. Consent was taken from all patients included in this project as per departmental protocol. All radiographs were taken in the department of radiology of Ziauddin Hospital. Panoramic and lateral Cephalometric films were acquired using PLANMECA Proline XC x-ray unit. They were obtained through a constant exposure of 9ma, 70kvp for 18sec. Evaluations of these radiographs were done by two trained operators working in the department of orthodontics of Ziauddin College of Dentistry.
Gonial angle was calculated from the intersection of two planes, i.e; plane of the ramus of the mandible and body of the mandible. There are three different methods to evaluate mandibular plane on cephalogram described by different orthodontic analysts, i.e; Charles H. Tweed, Cecil C. Steiner and William B.Downs. According to Tweed mandibular plane is formed by tangent to the lower border of the mandible, Steiner described it as a line connecting Gonion (Go) to Gnathion (Gn) & Downs mentioned it as a line joining
Gonion (Go) to Menton (Me) (Figure 1). On the

orthopantomogram Gonial angle was formed by the intersections of two tangents, one from the lower border of the mandible and another from the posterior border of condyle and ramus, on both sides and then taking an average value of the two (Figure 2).
All the data was then subjected to statistical analysis using SPSS version 23. Repeated measure ANOVA with Bonferroni correction was used to compare three methods of gonial angle formation on cephalogram with the method on orthopantomogram.

RESULTS
The study group consisted of 178 patients (54 males and 124 females) with various malocclusions and vertical relationships. Subject patients were divided into three groups according to the relation of mandibular plane with the SN plane, i.e; hyperdivergent – 36 subjects (9 males and 27 females), normodivergent – 64 subjects (25 males and 39 females) and hypodivergent – 78 subjects (20 males and 58 females).(Table: 1)

In hyperdivergent patients, the mean value of the gonial angle on the lateral cephalogram was 137.5o by Tweed’s,
130.2o by Steiner’s and 133.1o by Down’s and that on the panoramic radiograph was 131.6o . In normodivergent patients, the mean value of the gonial angle on the lateral cephalogram was 132.4o by Tweed’s, 125.3o by Steiner’s and 128.3o by Down’s and that on the panoramic radiograph was 126o. In hypodivergent patients, the mean value of the gonial angle on the lateral cephalogram was 127o by Tweed’s, 119.5o by Steiner’s and 122.5o by Down’s and that on the panoramic radiograph was 120.2o . (Table: 2) Repeated measure ANOVA was used to find the agreement between different methods of finding Gonial Angle on cephalogram and orthopantomogram. The mean – difference between the

values was found to be statistically significant (i.e; P = <0.05) after Bonferroni correction. (Table: 3)
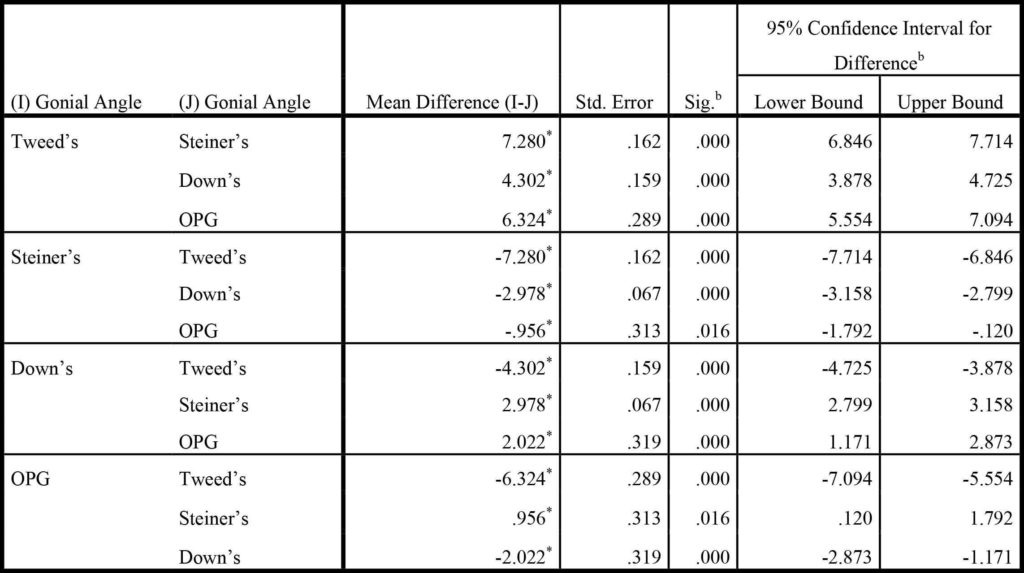
Based on estimated marginal means
*. The mean difference is significant at the .05 level.
b. Adjustment for multiple comparisons: Bonferroni.
DISCUSSION
The present study compared three methods of gonial angle formation on cephalogram with the method on Orthopantomogram, amongst three vertical facial groups. The knowledge of vertical facial growth and its implications with regard to orthopedic and orthodontic treatment is important especially in hyperdivergent and hypodivergent of skeletal pattern as it contributes to jaw rotation and facial aesthetics. It has been reported in the literature that a large gonial angle indicates a tendency towards posterior growth rotation of mandible and on the other hand small gonial angle indicates vertical growth of the condyles, giving a tendency to anterior growth rotation of the mandible.15-17 Furthermore, gonial angle also has a clear impact on profile changes and the position of the lower incisors. Researchers have conducted various studies to understand vertical facial growth and its implications in orthodontics.13-17 Lateral cephalogram are mostly used in routine orthodontic practice to evaluate a patient’s sagittal and vertical facial growth and dentoalveolar relationships before, during and after orthodontic treatment.14 17 Majority of patients do not require Lateral cephalograms unless they are planning to undergo orthodontic treatment. Conversely, Orthopantomogram are often taken throughout the life of a patient. Although compared to cephalograms, panoramic radiographs clearly differentiate left and right, due to the widely known magnification and distortion on the panoramic radiographs, the reliability of linear measurements are always debatable.13,14-16 Several researcher’s have compared the two types of radiographs for predicting cephalometric gonial angle.17-22
Bibi T in their study reported significant correlation between the cephalometric and panoramic values and concludes that panoramic radiography is as reliable as lateral cephalogram in predicting vertical facial pattern as assessed by gonial angle.18 In an other study statistically insignificant difference was found in the gonial angle measured by two different radiographic methods in three different types of occlusion.20 Thilagarani et al,21 in their study found statistically insignificant difference in gonial angle between the Tweeds mandibular plane on lateral cephalogram and panoramic radiograph in Class I, Class II and Class III patients. They concluded that the Tweeds mandibular plane is more reliable on lateral cephalogram to assess gonial angles in comparison to the other two mandibular planes of Steiner’s and Down.
The results of the present study are in contrast with the above studies. The difference in results could be due to difference in type of malocclusion as in the present study we compared the two types of radiographs in measuring gonial angle using three different mandibular plane in different vertical facial groups and found significant difference between two types of radiographs. Other researchers reported significant difference gonial angle obtained by the two different radiographs.13,16,23-25 They concluded that clinicians should be vigilant when predicting skeletal cephalometric parameters from panoramic radiographs, because of their lower predictability percentages.
Fisher -Brandies23 also reported significant difference in the gonial angle obtained by the two different radiographs. Adil et al13 in their hospital based survey on 80 patients traced gonial angle on radiographs (OPG and lateral Cephalometric readiograph) and found significantly different measurement of gonial angle between the two radiographs.
Araki et al., in 2015, found in their study that the gonial angle measurements on the panoramic radiographs were slightly smaller than on the lateral cephalometric radiographs.26 Nohadani et al.27 compared longitudinal vertical facial and dentoalveolar changes using panoramic radiographs with measurements on lateral cephalometric radiographs. They reported that panoramic dental radiographs are not useful for evaluating vertical facial parameters. The results of the present study are in agreement with the above studies. Based on the results of the present study, it is suggested that the similar study on large sample size should be conducted to find the agreement between three methods of gonial angle formation on cephalogram with the method on orthopantomogram, amongst three vertical facial groups.
CONCLUSION
The value of gonial angle determination on an Orthopantomogram was found to be different when compared with the three methods (Tweed’s, Steiner’s and down’s) of gonial angle determination on lateral cephalogram. Thus, orthopantomogram cannot be used as an alternative for gonial angle determination in orthodontic patients in various vertical facial groups. Furthermore, it cannot replace lateral cephalogram in the information contained in it.
CONFLICT OF INTEREST
None declared.
REFERENCES
- William R. Proffit, David M. Sarver, James L. Akerman. Diagnosis and treatment planning. In: William R, Henry W, David M. Contemporary orthodontics. Etiology of Malocclusion. 5th ed. St. Louis: Mosby. 2013. pp 150-219
- Weems RA. Radiographic Cephalometric Technique. In: Jacobson A, Jacobson RL, editors. Radiographic cephalometry: from basics to 3-D imaging. Hanover Park (IL): Quintessence Publishing Co.Inc. 2006. p. 33-44
- Nadkerny PV, Kumar DA, Nadkerny VD. Assessing reliability of mandibular planes in determining gonial angle
on lateral cephalogram and panoramic radiograph. Journal of Orthodontic Research. 2015;3:45. https://doi.org/10.4103/2321-3825.146358 - Caufiled PW. Tracing techniques and identification of landmarks. In: Jacobson A, Jacobson RL, editors. Radiographic cephalometry: from basics to 3-D imaging. Hanover Park (IL): Quintessence Publishing Co.Inc. 2006. p. 45-51.
- Jensen E, Palling M. The gonial angle: A survey. American Journal of Orthodontics. 1954;40:120-33.
https://doi.org/10.1016/0002-9416(54)90127-X - Jacobson A. Downs analysis.In: Jacobson A, Jacobson RL, editors. Radiographic cephalometry: from basics to 3- D imaging. Hanover Park (IL): Quintessence Publishing Co.Inc. 2006. P 63-70
- Jacobson A. Steiner analysis. In: Jacobson A, Jacobson RL, editors. Radiographic cephalometry: from basics to 3- D imaging. Hanover Park (IL): Quintessence Publishing Co.Inc. 2006. P 71-78.
- Shahabi M, Ramazanzadeh BA, Mokhber N. Comparison between the external gonial angle in panoramic radiographs and lateral cephalograms of adult patients with Class I malocclusion. J Oral Sci 2009; 51:425-9. https://doi.org/10.2334/josnusd.51.425
- Upadhyay RB, Upadhyay J, Agrawal P, Rao NN. Analysis of gonial angle in relation to age, gender and dentition status by radiological and anthropometric methods. J Forensic DentSci. 2012;4:29-33. https://doi.org/10.4103/0975-1475.99160
- Rubika J, Felicita AS, SivambigaV: Gonial Angle as an Indicator for the Prediction of Growth Pattern. World J Dent 2015;6:161 – 63. https://doi.org/10.5005/jp-journals-10015-1334
- Xiao D, Gao H, Ren Y. Craniofacial morphological characteristics of Chinese adults with normal occlusion and different skeletal divergence. Eur J Orthod 2011;33:198- 204. https://doi.org/10.1093/ejo/cjq064
- Larheim TA, Svanaes DB. Reproducibility of rotational panoramic radiography: mandibular linear dimensions and angles. American Journal of Orthodontics and Dentofacial Orthopedics 1986;90:45-51. https://doi.org/10.1016/0889-5406(86)90026-0
- Adil S, Awan MH, Khan I, Syed K. Comparison of the gonial angle measurements on Lateral Cephalogram and both hemispheres of Orthopantomogram. POJ 2016;7:48- 50.
- Mattila K, Altonen M, Haavikko K. Determination of the gonial angle from the orthopantomogram. Angle Orthod 1977;47:107-10.
- Sharma VK, Tandon P, Singh GK et al. Evaluation of Skeletal Patterns Using Panoramic Radiography. J Adv Res Dent Oral Health 2017;2:1-8. https://doi.org/10.24321/2456.141X.201701
- Nejad AM, Jamilian A, Meibodi SE, Hafezi L, Khosravi S, Cappabianca S, et al. Reliability of panoramic radiographs for determination of gonial and Frankfurt mandibular horizontal angles in different skeletal patterns. Stoma Edu J 2016;3:18-22.
- Akcam MO, Altiok T, Ozdiler E. Panoramic radiographs: a tool for investigating skeletal pattern. American journal of orthodontics and dentofacial orthopedics. 2003 Feb 28;123(2):175-81 https://doi.org/10.1067/mod.2003.3
- Bibi T, Rasool G, Khan H. Reliability of orthopantomogram in determination of gonial angle. Pak Oral Dent J 2017; l 37:248-51.
- Katti G, Katti C, Shahbaz S, Khan M, Ghali SR. Reliability of panoramic radiography in assessing gonial angle compared to lateral cephalogram in adult patients with Class I malocclusion. Journal of Indian Academy of Oral Medicine and Radiology. 2016 Jul 1;28(3):252 https://doi.org/10.4103/0972-1363.195668
- Zangouei-Booshehri M, Aghili HA, Abasi M, EzoddiniArdakani F. Agreement Between Panoramic and Lateral Cephalometric Radiographs for Measuring the Gonial Angle. Iran J Radiol. 2012; 9: 178-82. https://doi.org/10.5812/iranjradiol.8444
- Thilagarani, Purnima V. Nadkerny1, Kumar DA, Vidyesh D. Nadkerny. Assessing reliability of mandibular planes in determining gonial angle on lateral cephalogram and panoramic radiograph. Journal of Orthodontic Research 2015; 3: 45. https://doi.org/10.4103/2321-3825.146358
- Bhullar MK, Uppal AS, Kochhar GK, Chachra S, Kochhar AS. Comparison of gonial angle determination from cephalograms and orthopantoogram. Ind J Dent 2014; 5: 123-6. https://doi.org/10.4103/0975-962X.140820
- Fischer-Brandies H, Fischer-Brandies E, Dielert E. The mandibular angle in the orthopantomogram. Der Radiologe. 1984 Dec;24(12):547-9
- Akcam MO, Altiok T, Ozdiler E. Panoramic radiographs: a tool for investigating skeletal pattern. American journal of orthodontics and dentofacial orthopedics. 2003 Feb 28;123(2):175-81 https://doi.org/10.1067/mod.2003.3
- Araki M, Kiyosaki T, Sato M, Kohinata K, Matsumoto K, Honda K. Comparative analysis of the gonial angle on lateral cephalometric radiographs and panoramic radiographs. Journal of oral science. 2015;57(4):373-8. https://doi.org/10.2334/josnusd.57.373
- Araki M, Kiyosaki T, Sato M, Kohinata K, Matsumoto K, Honda K. Comparative analysis of the gonial angle on
lateral cephalometric radiographs and panoramic radiographs. J Oral Sci 2015; 57: 373-8. https://doi.org/10.2334/josnusd.57.373 - Nohadani N, Ruf S. Assessment of vertical facial and dentoalveolar changes using panoramic radiography. Eur J
Orthod. 2008;303:262-8 https://doi.org/10.1093/ejo/cjm106
1. Lecturer, Department of Orthodontics, Ziauddin College of Dentistry/Ziauddin University, Karachi.
2. Assistant Professor, Department of Orthodontics, Ziauddin College of Dentistry/Ziauddin University, Karachi.
3. MDS Trainee, Department of Orthodontics, Ziauddin College of Dentistry/Ziauddin University, Karachi.
Corresponding author: “Dr. Sarwat Memon †< sarwatmaqsood@yahoo.com >