


Zeeshan Qamar1Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â BDS, MSc
Tayyaba Fatima2Â Â Â Â Â Â Â Â Â Â Â Â Â Â BDS
Flowable composites are of low viscosity and a modification of small particle-filled and hybrid composites. They have reduced filler load and modified resin monomers which provide a consistency that allows the material to flow readily. They have better adaptability to cavity walls thus preventing microleakge.
HOW TO CITE: Qamar Z, Fatima T. Comparative Review Of Various Flowable Composites. J Pak Dent Assoc 2014; 23(1):11-14
INTRODUCTION
Restorative dentistry is going through a dynamic transition towards adhesive dentistry. A class of resin-composite systems known as ‘flowable composites’ has become an essential part of the restorative process since their introduction in the mid-nineties. These materials were developed in response to a demand from the clinicians for easy handling. They are characterized by having less filler load and greater portion of diluent monomers. Designed to be less viscous, and so the flowable composites offer a better adaptation to internal walls of the cavity, easier insertion and greater elasticity. Flowability of these materials allows them to be dispensed through injectable dispensers and simplifies easy placement procedures.
FLOWABLE COMPOSITES
Present day dental composites exhibit excellent aesthetics. Thus, due to this increasing demand, this has leaded to significant developments in terms of bond strength, adequate working time, shorter curing time and ease of use1. By the end of twentieth century, lowviscosity resin composite, generally known as flowable composites, were introduced amongst the variety of commercial commodities for restorative dentistry2. These flowable composites show two desirable clinical handling characteristics that were not present in composites until very recently. Firstly the material does not stick to the instruments, so the material can be easily filled in the cavity and secondly fluid injectability1.
Flowable composites were formed by keeping the same particle sizes of traditional hybrid composites, and by decreasing the filler content thus permitting increased resin to reduce the viscosity of the mixture1.
PROPERTIES OF FLOWABLE COMPOSITES
Wide ranges of flowable composite with different percentage of fillers (50%-70%/wt) are available and can be classified into low, medium or high viscosity3. Flowable composites are similar to traditional resin based fissure sealants. According to Sebastein, (2012) the former are said to have better mechanical and physical properties thus have been suggested to be used as pits and fissure sealants4. Lower filler loading results in greater polymerization shrinkage and lower mechanical properties compared to other hybrid composites5. Flowable composite also have low modulus of elasticity and their viscosity ranges from low to medium3,5. This suggests that these materials modulus of elasticity in 24 hours ranges from 2.8-6.0 GPa and thus they are not able to withstand the occlusal forces when used in bulk6. By decreasing the proportion of filler, flowable composites can easily adapt small cavity preparations. However their wear resistance is of major clinical concern as good wear resistance depends on increased filler load7. Complex viscosities of flowable composites decrease with increasing shear rate, showing a non-Newtonian behavior.4Flowable composites consist of less filler loading and the filler morphology is spherical due to which there is less shrinkage-strain values4. Their shrinkage-strain values at 23oC are 2.61-6.25%, and at 37oC range between 3.88-6.56%8. But in some flowable composite the spherical shaped filler particles have an advantage as they allow increased filler loading and enhance the fracture toughness value4. According to some in vitro studies flowable composites decrease restoration microleakage and the occurrence of voids9-11. This is mainly due to their ability to adapt well to the cavity walls and their stress-absorbing ability6. Flowable composites, as concluded in the study of Attar et al, (2003) have approximately 50% of the rigidity (elastic modulus) of the regular composites and approximately 80% of the flexural strength6.
In this article we will discuss the following flowable dental composites.
VERTISE FLOW
Flowable composites were brought on the market in the mid-nineties and have proven to be serviceable in a wide variety of clinical conditions.The company Kerr (Kerr, Corp, U.S.A) has developed Vertise TM flow as it’s first self adhering light cure flowable composite for direct restorations. Its formulation incorporated ‘optibond’ adhesion technology which eliminates the processes of, in no specific order; bonding, rinsing, priming and etching (Kerr, 2011).
This belongs to the 7th generation of dental composites as mentioned in table1, in which the triple mechanism
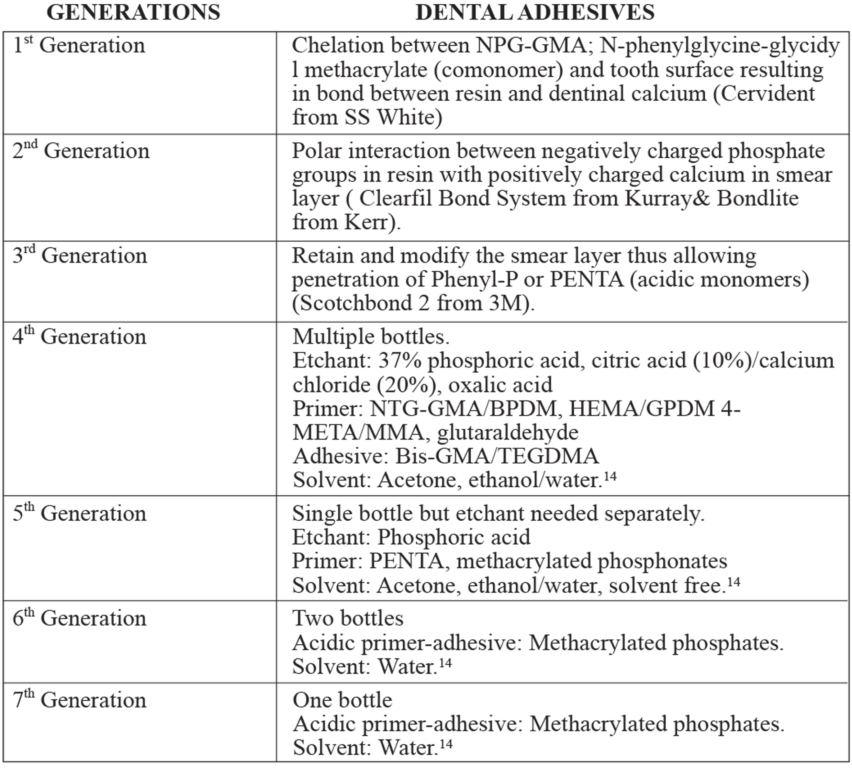
Table 1: Classification of dental adhesives. i.e. etchant, primer and adhesive are mixed together into one syringe. The glycerol-phosphate-di-methacrylate
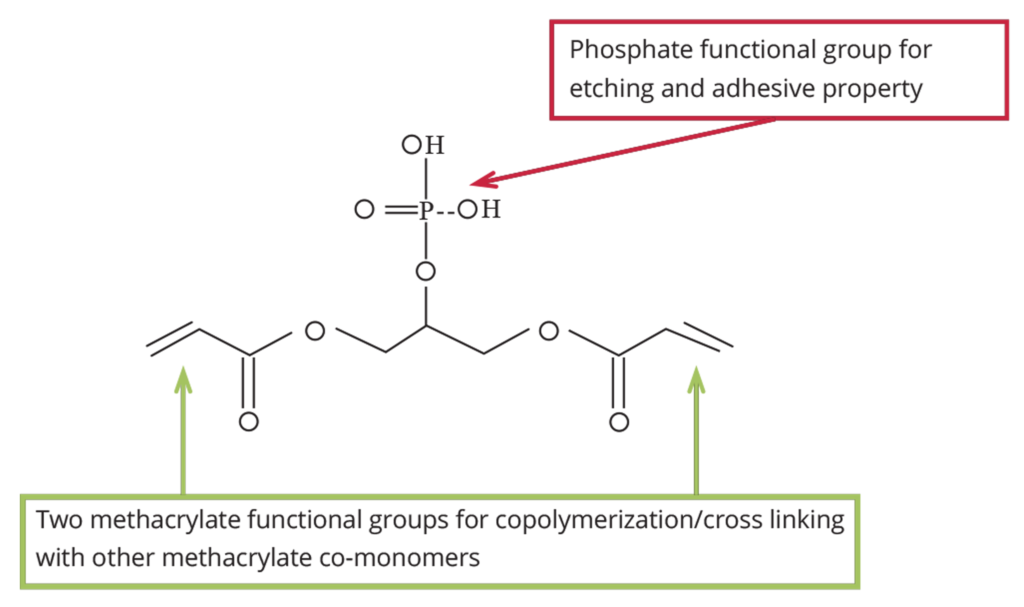
Figure 1:Â GPDM bonding in VertiseTM FLow (Kerr, 2011)
(GPDM introduced by Buonocore et al, 1956) between phosphate functional groups of GPDM monomer and calcium ions of enamel and dentine creates the bonding mechanism with the tooth structure where a chemical bonding is then attained as shown in Figure 112,13.Its composition includes GPDM and HEMA in the resin matrix and pre-polymerized barium glass filler, colloidal silica and ytterbium fluoride as filler constituents.
This material offers high bond strength, high mechanical strength and other physical attributes when compared to other traditional flowable composites3. It has multiple clinical implications and is available in nine different shades. It is a biocompatible and radiopaque product and bonds well to enamel, dentine, porcelain, metals, amalgams and composite3.
GRANDIO FLOW
Grandio flow is a nano-hybrid flowable type of composite. When compared to general hybrid-resin, it has the highest filler load4. Its resin to filler ratio is 1:6.7 (VOCO, Grandio Flow). Filler morphology of Grandio under the SEM showed higher irregular shaped particles4. Fillers present in this material are two-thirds inorganic
fillers and the resin part consist of Bis-GMA, TEGDMA and HEDMA.
Grandio flow offers various outstanding physical properties along with its less polymerization shrinkage that is 1.57%. Its properties include good wettability, high compressive and transverse strength, less cytotoxity and good abrasion resistance15. Moreover, the nanoparticles create a network effect within the matrix that increases tensile strength, wear resistance and good flow properties16. Vickers hardness test by the Durimet gave the result of 59.9VHN, which was higher than the Premise flowable.
PREMISE FLOWABLE
Premise flowable composite (Kerr, Corp, U.S.A) is a medium viscosity, light cured, nano-hybrid composite. This material is used after the application of ‘optibond/FL’ or ‘optibond solo plus’ in the cavity. The material also poses a unique property of releasing fluoride and radiopacity. It contains more regular spherically shaped filler particles. The percentage of filler content by weight in Premise flowable is 72.5%4. Premise flowable contains the trimodal filler system and resin part consists of ethoxylated bis-phenol-A-dimethacrylate.
Premise flowable composite is based on the trimodal technology, which comprises pre-polymerised filler (it is a of blend low shrinkage resin, barium glass and 0.02 micron filler-), point-4 filler and 0.02 micron filler. Due to this technology, this material shows; less shrinkage, optimal handling, good polish, durability, good mechanical strength and good wear resistance compared to other flowable composites.
HYDROXYETHYL METHACRYLATE (HEMA)
Hydroxyethyl methacrylate (HEMA) Figure 2 is a hydrogel; it is hydrophilic in nature and potentially biocompatible. Thus it’s of great interest in the field of Hydrophobic End

Figure 2: Chemical structure of Hydroxyethyl methacrylate
biomaterial sciences and manufacturing soft contact lenses17. Hydrogels being hydrophilic polymers, absorb 10-20% water, being a thousand times more than their dry weight. They are chemically stable, may degrade and finally breakdown and disintegrate17. The elasticity of these hydrogels can be improved by altering their structure and by adding cross-linking agents18,19. Most commonly used cross-linking agent is ethylene glycol dimethacrylate20.
The nature of water in the hydrogel can determine the permeation of nutrients in and out of the gel. Hoffman described water absorption by HEMA as follows: A dry hydrogel starts to absorb water; this first water enters the matrix and hydrates the matrix with the most polar (hydrophilic group) resulting in ‘primary bound water’17. These polar groups, after being hydrated swell and expose hydrophobic groups; these also interact with molecules of water leading to ‘secondary bound water’ (hydrophobically bound water). Total bound water is formed by the combination of primary and secondary bound waters. Equilibrium is reached when further swelling is opposed by covalent/physical cross-links, leading to an elastic network of retraction forces. This additional water that is imbibed becomes saturated and is called the ‘free’ or ‘bulk water’. It is this free water that occupies the gaps between network chains and voids17. Thus HEMA being one of the important components of Vertise flow has made this material a subject to study.
DISCUSSION
The composites chosen for this study are marketed in the UK as low viscosity, self-adhering composites, suitable for pits and fissure sealants, repair of marginal defects, liners in deep cavities, class-v restoration and paediatric dentistry.
The company Kerr has formulated a self-adhering, low viscosity nano-hybrid composite known as Vertise TM Flow. It includes the Optibond technology and eliminates the steps of etching/priming/bonding. The bonding mechanism of this material with the tooth structure is a chemical bond achieved via the GPDM phosphate functional groups and calcium ions of the enamel and dentine. According to the company’s, this material offers high bond strength, high mechanical strength and other physical attributes comparable to other traditional flowable composites. Vertise TM Flow is a biocompatible and radiopaque material and bonds well to different substrates including enamel, dentine, porcelain, metals, amalgam and composite.
Vertise TM Flow has been a subject of this study here due to its composition containing HEMA and low filler loading (compared with Grandio Flow and Premise Flow). HEMA is a hydrophilic monomer which absorbs water and could potentially decrease the properties of the material21.
The other materials used in the study were Grandio Flow and Premise Flow. Both these are low viscosity flowable composites. The difference between them and Vertise TM Flow is that they do not contain HEMA. These are nano-hybrid composites, and their filler content by weight is 72.5% in Premise Flow and 80.2% in Grandio Flow. They both have good physical and mechanical properties but PF has an added advantage of releasing fluoride and having a higher radiopacity than Grandio Flow. These materials are in used in this study for comparisons purposes.
CONCLUSION
Flowable composites are of low viscosity and a modification of small particle-filled and hybrid composites. They have reduced filler load and modified resin monomers which provide a consistency that allows the material to flow readily. They have better adaptability to cavity walls thus preventing microleakge.
REFRENCES
- Tecco S, Traini T, Caputi S, Festa F, de Luca V, D’Attilio M. A new one-step dental flowable composite for orthodontic use: an in vitro bond strength study. The Angle Orthodontist. 2005;75:672-677.
- Labella R, Braden M, Davy KW. Novel acrylic resins for dental applications. Biomaterials. 1992; 13:937-943.
- Sabbagh J, Souhaid P. Vertise & trade; Flow Composite; A Breakthrough in Adhesive Dentistry. Oral health group. 2011;3:22-27.
- Beuna S, Bailly C, Devaux J, Leloupa G. Physical, mechanical and rheological characterization of resinbasedpit and fissuresealants compared to flowableres in composites. Dent Mater. 2012; 28:349-359.
- Labella R, Lambrechts P, Van Meerbeek B, Vanherle G. Polymerization shrinkage and elasticity of flowable composites and filled adhesives. Dent Mater. 1999;15: 128-137.
- Attar N, Tam LE, McComb D. Flow, strength, stiffness and radiopacity of flowable resin composites. J Canadian Dent Assoc. 2003; 69:516-521.
- Clelland NL, Pagnotto MP, Kerby RE, Seghi RR. Relative wear of flowable and highly filled composite. J Prosth Dent. 2005;93:153-157.
- Baroudi K, Silikas N, Watts DC. Time-dependent visco-elastic creep and recovery of flowable composites. European J Oral Sci. 2007;115:517-521.
- Payne JH. The marginal seal of class II restorations: flowable composite resin compared to injectable glass ionomer. J ClinPediatr Dent 1999; 23:123-130.
- Ferdianakis K. Microleakage reduction from newer esthetic restorative materials in permanent molars. J Clin Pediatr Dent 1998;22:221-229.
- Malmstrom H, Schlueter M, Roach T, Moss ME. Effect of thickness of flowable resins on marginal leakage in class II composite restorations, Oper Dent. 2002;27:373-380.
- Buonocore M, wileman W, BrudevoldF. A report on a resin composition capable of bonding to human dentin surfaces. J Dent Res. 1956;35:846-851.
- Wei YJ, Silikas N, Zhang ZT, Watts DC. Hygroscopic dimensional changes of self-adhering and new resinmatrix composites during water sorption/desorption cycles. Dent Mater. 2011; 27:259-266.
- Powers JM and Sakaguchi RL, Craig’s Restorative Dental Materials 12th 2006, Elsevier
- Sigusch BW, Pflaum T, Völpel A, Gretsch K, Hoy S, Watts DC, Jandt KD. Resin-composite cytotoxicity varies with shade and irradiance. Dent Mater. 2012;28:312-319.
- Sideridou ID, Karabela MM, VouvoudiECh. Physical properties of current dental nanohybrid and nanofill lightcured resin composites. Dent Mater. 2011;26: 599-607.
- Hoffman AS . Hydrogels for biomedical applications. Advance drug delivery reviews. 2002;54:3-12.
- Rao JK, Ramesh DV, Rao KP. Implantable controlled delivery systems for proteins based on collagen–pHEMA hydrogels .Biomaterials. 1994;15:383.
- Carlos Peniche, Ma Eugenia Cohen.Water sorption o f f l e x i b l e n e t w o r k s b a s e d o n 2 hydroxyethylmethacrylate-triethylenglycoldimethacrylate copolymers. Polymer. 1997;38:5977-5982
- Wichterle O. Hydrogels, in Encyclopedia of Polymer Science and Technology, Vol. 15 ed. H. F. Mark and N.G. Gaylord, Wiley, 1971, p.273.
- Downes S, Patel MP, Di Silvio L, Swai S, Davy KWM, Braden M. Modifications of the hydrophilicity of heterocyclic methacrylate co-polymers for protein release. Biomaterials. 1995;16:1417-1421.
- Head of the Oral Biology Department Ziauddin University Karachi, Pakistan.
- Department of Oral Biology University of Malaya Kuala lumpur, Malaysia.
Corresponding author: “Dr. Zeeshan Qamar†< zeeshan.qamar@ymail.com >