
Prevalence of Early Childhood Caries (ECC)
INTRODUCTION
The American Dental Association defines early childhood caries (ECC) presence of black lesion (cavitated or non-cavitated) in any primary tooth of a preschooler, 0-71 months old.”1, 2 It is also known as babys bottle’ or ‘nursing bottle’ caries. Mostly, it occurs on labial surfaces of maxillary anterior teeth but any other tooth can be affected as well.. It is an infectious, chronic disease caused by a number of factors which affects 1-17% children in developed and 70% children in under-developed countries.3 The triad for caries to occur includes tooth surface, cariogenic bacteria and fermentable carbohydrates.4 Several behavioral factors and demographics appear to be determinants of ECC which include limited access to care, finances and oral health education. In addition, the value that parents place on primary teeth and views on prolonged bottle-feeding have also been identified as predictors of caries-risk.2
It is the most prevalent unmet health need especially among children in the developing countries. Left untreated, ECC impacts the quality of life to an extent similar to other systemic diseases and may lead to excruciating dental pain and infection.5
Highest prevalence of early childhood caries is reported from Africa and South-East Asia.6 In India, prevalence of this disease among children between 8–48 months was reported as 44%.7. One study in Sri Lanka reported the incidence of ECC to be 23% in children of age 1-2 years.8 While in North America the prevalence of ECC ranges from 11-72%.9 In Pakistan difference studies stated the prevalence of ECC from 27.9% to 51%10 11.
A valuable tool can be prepared by knowing the frequency and prevalence of ECC and its contributing factors, which will help in planning and implementing health care programmes. Such data is rarely found especially when it comes to a developing country like Pakistan. Aimed at focusing 6-36 months old children, this study is meant to assess the frequency of ECC on the basis of various risk factors.
METHODOLOGY
This cross-sectional survey was conducted at Outpatient Department (OPD) of Pediatrics, Shaikh Zayed Medical Complex Lahore, for 06 months. A total of 400 children from 6-36 months of age with no physical or mental illness were included in the study. Verbal consent from parents was obtained prior to including children in the study and an interviewer administered questionnaire asked mother's education, oral hygiene aids, feeding method and pattern and sugar consumption by the child. After explaining the aim of study, oral cavity of children and their mothers was examined under good light using disposable wooden spatulas. The deft and DMFT was calculated after examination. Data collection and examination was done by three dental surgeons to facilitate the process.
The completed questionnaires were collected and total responses for each item were tabulated. Data was entered and analyzed by using statistical software, Statistical Package for Social Sciences (SPSS) version 21.0. Chi square test was applied as test of significance. For all analysis p value ≤0.5 was taken as significant.
RESULTS
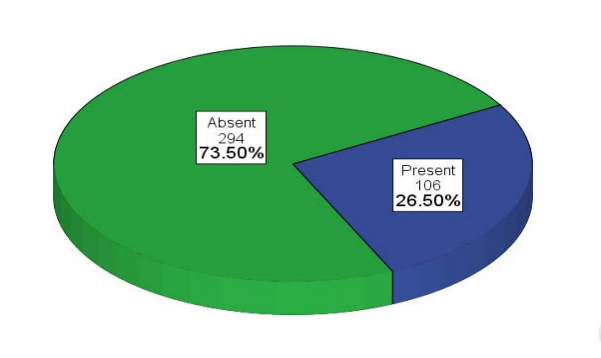
The prevalence of ECC in our study was 26.5% in all children of age 6-36 months with mean deft value of 0.60± 1.13 and mean DMFT value of 1.60±1.88 (see Table 1).
 Table 1. Clinical assessment of children and mothers regarding caries (n=400).
Table 1. Clinical assessment of children and mothers regarding caries (n=400).
 Prevalence of ECC in children
Prevalence of ECC in children
The comparative analysis showed that in age >12 months, the frequency of ECC was significantly high (P<0.05) (see Table 3), however there was no difference in both genders for ECC (P>0.05). While feeding method and pattern, sugar addition to bottle milk, dietary habits and mothers education (P>0.05) had significant impact on frequency of ECC (p<0.05) (see Table 2).
DISCUSSION
ECC is a major public health problem that continues to affect toddlers and small children worldwide with prevalence varying among populations. Many studies on ECC have been conducted to identify the etiology, prevalence, risk factors and treatment of this disease over the past 40 years12.
 Table 2. Comparison of both genders for different characteristics related to caries.
Table 2. Comparison of both genders for different characteristics related to caries.
This study also adds to the evidence of existing knowledge. The study was conducted in the Outpatient Department of Pediatrics, Sheikh Zayed Medical Complex Lahore, among 400 children of age between 6-36 months. The study determined that almost one fourth, 26.5% of children had ECC. This shows a slight variation from a few previous studies done in Pakistan. In a study conducted at Tertiary Care Hospital, Karachi in 2010, the reported prevalence was 50.1% in children attending dental OPD.13 While a research by Sufia et al., calculated the dental caries prevalence about 40.1% among the children of 3-5 years.14 Both of these were community based holistic studies which would explain the difference in result from our study.
The present study reported that statistically significant (82.5%) children with ECC were either bottle fed or taking both. This is supported by a similar study conducted in the department of Child Dental Health at University Teaching Hospital Lagos, Nigeria which showed that children who were solely bottle-fed had a caries prevalence of 33% greater than those who were solely breastfed (15.7%) or taking both (25.3%)15.
 Table 3. Comparison of mean deft in children of different age groups.
Table 3. Comparison of mean deft in children of different age groups.
It was also apparent in our study that in the age >12 months, the prevalence of ECC was significantly high (P<0.05), contrary to a study conducted in Karachi where age had no significant impact on ECC.16 However, other studies conducted in Peshawar10 and Sri Lanka17 showed higher frequency of dental caries with age.
Gender had no significant role in the development of ECC. These findings are in agreement with other studies conducted in Peshawar10 and Karachi.18.
In our study, mother's education which appeared to be directly influencing the child's dietary habits and oral hygiene aids was found to be indirectly proportional to the prevalence on ECC. This is supported by the analysis of another study conducted in India19 where the children of less educated and illiterate mothers had more dental caries.
CONCLUSION
Frequency of ECC in patients presenting to Pediatrics Department of Sheikh Zayed Medical Complex. Medical Complex was found to be 26.5%. Feeding habits and mother's education was found to have a significant association with frequency of dental caries.
ACKNOWLEDGEMENT
Pediatrics Department of Shaikh Zayed Medical Complex. Miss Iqra Waheed, Consultant Biostatistician.
AUTHORS’ CONTRIBUTION
Dr. Iqura Khan Assisted in data collection and write up.
Dr. Raza Javed Assisted in data collection.
Dr. Rizwan Mahmood Assisted in data collection.
Dr. Faiza Awais Assisted in write up.
DISCLOSURE
NONE declared.
REFERENCES
- Drury TF, Horowitz AM, Ismail AI, Maertens MP, Rozier RG, Selwitz RH. Diagnosing and reporting early childhood caries for research purposes: a report of a workshop sponsored by the National Institute of Dental and Craniofacial Research, the Health Resources and Services Administration, and the Health Care Financing Administration. J Pub Health Dent 1999; 59(3): 192-97.
- Kumarihamy SL, Subasinghe LD, Jayasekara P, Kularatna SM, Palipana PD. The prevalence of Early Childhood Caries in 1-2 yrs olds in a semi-urban area of Sri Lanka. BMC Res Notes 2011; 4: 336.
- Ghazal TSA. Prevalence, Incidence and Risk Factors for Early Childhood Caries Among Young African-American Children in Alabama. J Public Health Dent 2013; 75(1): 42-8.
- van Loveren C, Broukal Z, Oganessian E. Functional foods/ingredients and dental caries. Eur J Nutr 2012; 51(2): 15-25.
- Goettems ML, Ardenghi TM, Demarco FF, Romano AR, Torriani DD. Children’s use of dental services: influence of maternal dental anxiety, attendance pattern, and perception of children’s quality of life. Commun Dent Oral Epidemiol 2012; 40(5): 451-58.
- Kumar VD. Early childhood caries – an insight. J Int Oral Health 2010; 2(1):1-9
- Ribeiro NM, Ribeiro MA. Breastfeeding and early childhood caries: a critical review. J Pediatr 2004; 80(5): s199-s210.
- Shahim FN. Factors of risk ealey childhood caries in a selected district in Sri Lanka. Colombo, Sri Lanka: University of Colombo; 2003.
- Low W, Tan S, Schwartz S. The effect of severe caries on the quality of life in young children. Pediatr Dent 1998; 21(6): 325-26.
- Saleem U, Bibi S, Jamil B. Early childhood caries and its relationship with different risk factors in preschool children. J Postgrad Med Inst 2015; 29(1):24-7.
- Dawani N, Nisar N, Khan N, Syed S, Tanweer N. Prevalence and factors related to dental caries among pre-school children of Saddar town, Karachi, Pakistan: a cross-sectional study. BMC Oral Health 2012; 12(1):59.
- Peretz B, Eidelman E. New insights into early childhood caries and strategies for prevention. In: Gluck GM, Morganstein WM, editors. Jong’s community dental health. Philadelphia: Mosby; 2003. p.157-59.
- Inayat N, Mujeeb F, Shad MA, Rashid S, Hosein T. Early childhood caries, bottle-feeding, socioeconomic status, cariogenic snacks. J Pak Dent Assoc 2010; 19(1): 34-41.
- Sufia S, Chaudhry S, Izhar F, Syed A, Mirza BA, Khan AA. Dental Caries Experience in Preschool Children—Is It Related to A Child’s Place of Residence and Family Income? Oral Health Prevent Dent. 2011; 9(4): 375-79.
- Olatosi O, Sote E. Association of early childhood caries with breastfeeding and bottle feeding in southwestern Nigerian children of preschool age. J West Afr Coll Surg 2014; 4(1): 31-53.
- Charani A, Mohsin S, Sufia S, Khan A. Prevalence of early childhood caries among 3-5-year old children of Clifton, Karachi. J of Pak Dent Assoc 2011; 20: 89-92.
- Perera PJ, Abeyweera NT, Fernando MP, Warnakulasuriya TD, Ranathunga N. Prevalence of dental caries among a cohort of preschool children living in Gampaha district, Sri Lanka: A descriptive cross sectional study. BMC Oral Health 2012; 12(1):49.
- Inayat N, Mujeeb F, Shad M, Rashid S, Hosein T. Experience of early childhood caries in children at Fatima Jinnah dental college and hospital, Karachi and its relationship with feeding practices. J Pak Dent Assoc 2010; 19: 35-40.
- Prakash P, Subramaniam P, Durgesh B, Konde S. Prevalence of early childhood caries and associated risk factors in preschool children of urban Bangalore, India: A cross-sectional study. Eur J Dent 2012; 6(2): 141.